Background
There is growing evidence suggesting that beyond the acute phase of SARS-CoV-2 infection, people with COVID-19 could experience a wide range of post-acute sequelae, including diabetes. However, the risks and burdens of diabetes in the post-acute phase of the disease have not yet been comprehensively characterised. To address this knowledge gap, we aimed to examine the post-acute risk and burden of incident diabetes in people who survived the first 30 days of SARS-CoV-2 infection.
Methods
In this cohort study, we used the national databases of the US Department of Veterans Affairs to build a cohort of 181 280 participants who had a positive COVID-19 test between March 1, 2020, and Sept 30, 2021, and survived the first 30 days of COVID-19; a contemporary control (n=4 118 441) that enrolled participants between March 1, 2020, and Sept 30, 2021; and a historical control (n=4 286 911) that enrolled participants between March 1, 2018, and Sept 30, 2019. Both control groups had no evidence of SARS-CoV-2 infection. Participants in all three comparison groups were free of diabetes before cohort entry and were followed up for a median of 352 days (IQR 245–406). We used inverse probability weighted survival analyses, including predefined and algorithmically selected high dimensional variables, to estimate post-acute COVID-19 risks of incident diabetes, antihyperglycaemic use, and a composite of the two outcomes. We reported two measures of risk: hazard ratio (HR) and burden per 1000 people at 12 months.
Findings
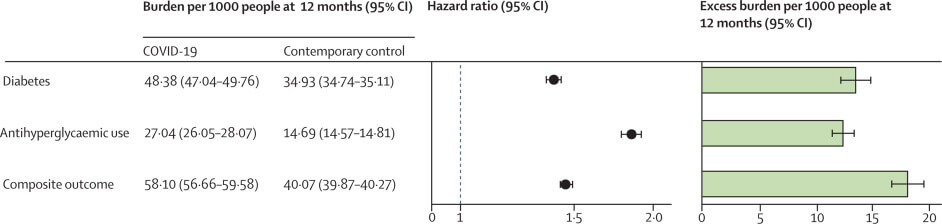
In the post-acute phase of the disease, compared with the contemporary control group, people with COVID-19 exhibited an increased risk (HR 1·40, 95% CI 1·36–1·44) and excess burden (13·46, 95% CI 12·11–14·84, per 1000 people at 12 months) of incident diabetes; and an increased risk (1·85, 1·78–1·92) and excess burden (12·35, 11·36–13·38) of incident antihyperglycaemic use. Additionally, analyses to estimate the risk of a…

